

The effect of short-term and long-term coronavirus quarantine on physical performance and injury incidence in high-level soccer
Summary of several aspects considered in the paper recently published in the Journal Soccer & Society. (click on the image to go the website)

Guerrero-Calderón B (2020) The effect of short-term and long-term coronavirus quarantine on physical performance and injury incidence in high-level soccer, Soccer & Society. DOI: 10.1080/14660970.2020.1772240
With this article, I have managed to gather the opinion of international soccer experts on the effect of short- (ST) and long-term (LT) QRT on physical performance and injury incidence in high-level soccer players, using open-ended questions in order to encourage the expression of unrestricted opinion. In this way, the text aims to provide the reader, whether strength & conditioning coach (S&C), physiotherapist, children’s coach or sport enthusiastic, from a practical perspective with a compilation and relationship of knowledge to understand how the coronavirus quarantine may affect the physical performance of high-level players based on the extensive experience and broad careers of conditioning area professionals in top-level soccer teams around the world together with the knowledge provided by research.
Effect on physical performance
Due to the forecast of a congested competition calendar after QRT, it will be necessary to optimize players’ physical performance to withstand the high physical demands of high-level soccer. The experts reported that individualized home training programs (HTP) have been developed for all players during QRT, in addition to specific nutrition plans. Nonetheless, despite the fact that all players are expected to act professionally and perform their HTPs, coinciding with the research, experts consider that there will be an irremediable physical performance decrease in the ST and, consequently, an increase in risk factors (RFs). The experts considered that the QRT will lead to negative changes in body composition in ST (Torreño & Owen), decrease in cardiorespiratory capacity of players (Aceña) and decrease in the capacity to generate strength, especially in soccer-specific muscle contractions and effort (Campos, Jiménez Rubio & Djaoui).
Injury incidence
In line with the literature, all the experts agreed that muscular injuries will be the most prevalent. Dr. Owen believes that most injuries will occur on reactive actions during turns. For Dr. Torreño, the main RF will be the loss of muscle mass and strength. Table 1 shows the most common muscular injuries considered by experts.
| Injury/Location | Experts |
| Muscle – Hamstrings | Aceña, Campos, Sala, Torreño, Owen |
| Muscle – Quadriceps | Aceña, Campos, Jiménez Rubio, Sala, Torreño, Owen |
| Muscle – Adductors | Campos, Sala, Owen |
| Muscle – Calf | Jiménez Rubio, Owen |
| Groin pain | Sala |
| Tendinopathies | Sala |
| Joints | Granero |
| Hernias | Owen |
Lluis Sala believes that different injuries will occur when the team returns to training and when competition begins: as soon as teams resume training, the flexor and adductor hip injuries, in addition with overuse injuries such as tendinopathy and groin pain. On the other hand, once competition starts and due to the congested match schedule, teams will increase the incidence rate of muscle injuries, without betting on a specific area. Based on the research, I believe overuse injuries RF on adductors muscles and groin pain will be high from the second or third week onwards if there is not enough preparation time to progressively increase the load before the start of competition.
Similarly, Ángel Aceña suggests two possible scenarios that might change the injury epidemiology: if the team does not have enough preparation time before returning to competition the hamstrings strain will be the most prevalent injuries; if, on the contrary, the teams can provide 3-4 weeks of preparation, the excessive training load may cause a greater number of quadriceps strain injuries.
Several experts agreed that there is a need for in-depth knowledge and exhaustive and individualized daily monitoring of players to adapt training and match load in order to identify the players best prepared for competition (Torreño, Jiménez Rubio, Granero, Sala & Djaoui). For Ángel Aceña & Dr. Torreño the biggest challenge for teams will not be to restore fitness capacity, but to cope with a very congested match calendar which will complicate players’ recovery process. Therefore, load individualization, together with the control and dosage of minutes of play together with rotation of player will be key elements in load management for S&C Coaches (Aceña, Campos, Owen & Granero), especially for teams also competing at international level, e.g. UEFA Champions League or Europa League (Jiménez Rubio).
Physical performance & injury risk relationship
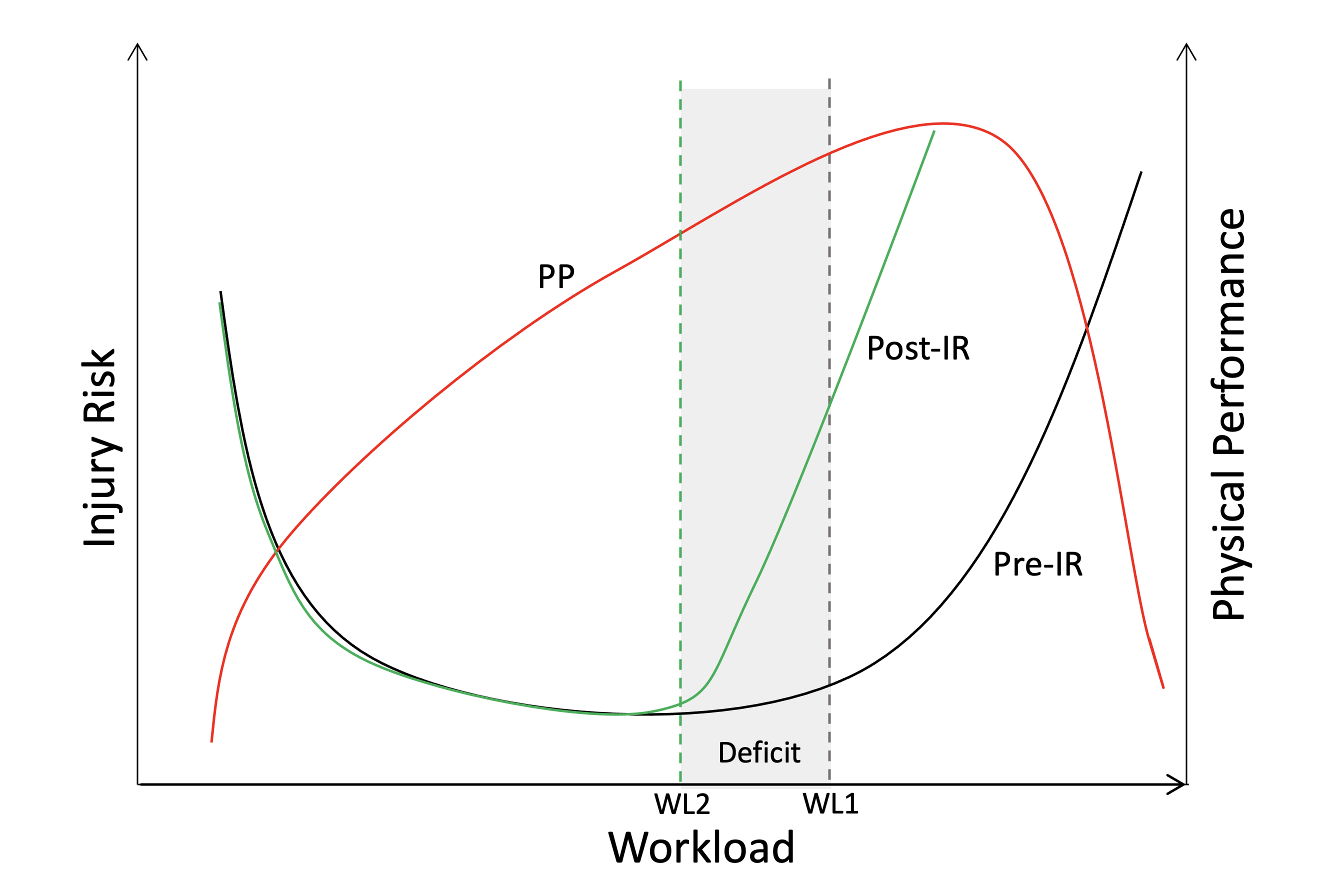
Figure 1 shows a subjective interpretation of the relationship between physical performance, workload bearing capacity and injury risk, differentiating the periods before QRT (pre-IR) and when retraining after QRT (post-IR). At first, it is important to note that a greater workload does not necessarily means better physical performance. However, it is well known that high-level soccer requires excellent physical capacity of players in order to cope with the demands of competition (Bradley et al., 2016). Therefore, players with good fitness (represented by the PP line) will be able to withstand very high loads with lower risk of injury. When the workload is increased to improve physical performance, there is a ‘relative point’ of load, which currently cannot be known since there are many contributing factors such as accumulated load (S. Malone, Owen, Mendes, et al., 2017), locomotion activity and intensity (Martín-García, Gómez Díaz, Bradley, Morera, & Casamichana, 2018; Owen, Djaoui, Newton, Malone, & Mendes, 2017), mood and sleep quality (Carling et al., 2018), previous fatigue (Bradley & Noakes, 2013) or contextual factors (Andrzejewski, Chmura, Konefał, Kowalczuk, & Chmura, 2017; Brito, Hertzog, & Nassis, 2016; Curtis et al., 2019; Rago, Rebelo, Krustrup, & Mohr, 2019), among others, in which there is an exponential increase in injury. In addition, rapid or excessive load increases may involve a substantially increased RF.
Therefore, the training-free period of QRT will cause a deficit (represented by the grey shaded area) of the capacity to cope with greater loads (Gabbett, 2016) and increase the RF (represented by the left yield RF curve shift [post-RF]). A progressive load increase will help players to attain greater capacity to cope with the workload thus reducing load deficit caused by QRT and consequently improving the physical performance and decreasing the injury RF (flattening and right-shift of the curve, from post-IR to pre-IR). To minimize the left-shift of the curve and therefore produce a smaller load deficit that players are able to cope without an exponential increase in RF, players should maintain an adequate strength capacity during QRT, mainly in the lower limbs, to mitigate the muscle damage that will occur when they return to training (Torreño).
Return to training
There are several opinions regarding the starting point after QRT: an initial workload about 50-60% (Dr. Owen); start with the ‘minimum dose of effective training-load’ and build a progressive adaptation (Aceña & Jiménez Rubio); and other experts consider that players’ physical capacity should be tested as soon as training resumes (Djaoui, Jiménez Rubio & Sala).
On the other hand, several experts considered that group training sessions after QRT should be completely contextualized with respect to the game from the beginning by integrating the conditional goals into the tasks to improve game pace (Torreño & Campos). Therefore, in addition to improving players’ physical performance by generating new and game-specific muscle adaptations, the injury RF will be reduced and recovery process will improve due to the positive relationship between players’ capacity to generate strength and the reduction of post-match muscle damage markers (Akenhead & Nassis, 2016; J. Malone et al., 2015; Owen et al., 2017). However, players should undertake individualized training sessions that complement the team training in order to enhance possible weaknesses and facilitate the recovery process.
Long-term affectation
There are many doubts about how the QRT will affect LT (Jiménez Rubio, Granero, Sala, Torreño & Djaoui). For Dr. Jiménez Rubio, the current focus is on assessing how the QRT period has affected players in order to design the applicable individualized training programs for preventing ST injuries. Afterwards, different training contexts may be handled to prevent LT injuries. Finally, the players psychological state will be of paramount importance (Granero, Djaoui & Jiménez Rubio).
Conclusions & Recommendations
- The QRT will highly negative affect the players’ physical capacity. In addition, it is also expected a reduction on the technical-tactical performance and game pace due to the decontextualization of QRT period.
- All the participating experts are in agreement with the need to dispose a minimum of 3 training weeks before start to compete.
- It will be necessary to dose the minutes of play by player and carry out the timely substitutions. In this sense, it might be interesting to be able to exceptionally perform a greater number of substitutions during the match.
- Pre-QRT player data should not be used as reference values (e.g., accumulated load).
- HTPs should mainly focus on HIT and strength and power training.
- It is very important to include the eccentric training into the strength program of QRT to reduce the muscle damage when returning to training.
- According to experts, hamstring and quadriceps strains will be the most prevalent injuries. In addition, overused injuries in adductors muscles and groin pain may also have high injury rate if there are rapid load increases.
- The main injury RF will be the lack of specific-soccer locomotion activity (high-intensity, sprints, accelerations and decelerations) and ball hitting during QRT.
- The role of technical staff will be decisive in the workload management to cope a congested competitive calendar.
- Some experts consider that the psychological state and mood of players will be affected due to players will be under very significant strain.
Acknowledgments
I sincerely thank the physical performance and injuries experts collaborating in this study; Ángel Aceña, Dr. Campos, Dr. Jiménez Rubio, Paulino Granero, Lluis Sala, Dr. Torreño, Dr. Djaoui and Dr. Owen; for their excellent contributions and exchange of knowledge and broad work experience in elite-level soccer.
References (only in this post)
- Akenhead, R., & Nassis, G. P. (2016). Training Load and Player Monitoring in High-Level Football: Current Practice and Perceptions. International Journal of Sports Physiology and Performance, 11(5), 587–593.
- Andrzejewski, M., Chmura, P., Konefał, M., Kowalczuk, E., & Chmura, J. (2017). Match outcome and sprinting activities in match play by elite German soccer players. The Journal of Sports Medicine and Physical Fitness, 58(6), 785–792.
- Bradley, P. S., Archer, D. T., Hogg, B., Schuth, G., Bush, M., Carling, C., & Barnes, C. (2016). Tier-specific evolution of match performance characteristics in the English Premier League: it’s getting tougher at the top. Journal of Sports Sciences, 34(10), 980–987.
- Bradley, P. S., & Noakes, T. D. (2013). Match running performance fluctuations in elite soccer: Indicative of fatigue, pacing or situational influences? Journal of Sports Sciences, 31(15), 1627–1638.
- Brito, J., Hertzog, M., & Nassis, G. P. (2016). Do Match-Related Contextual Variables Influence Training Load in Highly Trained Soccer Players? Journal of Strength and Conditioning Research, 30(2), 393–399.
- Carling, C., Lacome, M., McCall, A., Dupont, G., Le Gall, F., Simpson, B., & Buchheit, M. (2018). Monitoring of Post-match Fatigue in Professional Soccer: Welcome to the Real World. Sports Medicine, 48(12), 2695–2702.
- Curtis, R. M., Huggins, R. A., Benjamin, C. L., Sekiguchi, Y., Adams, W. M., Arent, S. M., … Casa, D. J. (2019). Contextual Factors Influencing External and Internal Training Loads in Collegiate Menʼs Soccer. Journal of Strength and Conditioning Research, 1.
- Gabbett, T. J. (2016). The training—injury prevention paradox: should athletes be training smarter and harder? British Journal of Sports Medicine, 50(5), 273–280.
- Malone, J., Di Michele, R., Morgans, R., Burgess, D., Morton, J., & Drust, B. (2015). Seasonal training-load quantification in elite English premier league soccer players. International Journal of Sports Physiology and Performance, 10(4), 489–497.
- Malone, S., Owen, A. L., Mendes, B., Hughes, B., Collins, K., & Gabbett, T. J. (2017). High-speed running and sprinting as an injury risk factor in soccer: Can well-developed physical qualities reduce the risk? Journal of Science and Medicine in Sport, 21(3), 257–262.
- Martín-García, A., Gómez Díaz, A., Bradley, P. S., Morera, F., & Casamichana, D. (2018). Quantification of a professional football team’s external load using a microcycle structure. Journal of Strength and Conditioning Research, 32(12), 3511–3518.
- Owen, A. L., Djaoui, L., Newton, M., Malone, S., & Mendes, B. (2017). A contemporary multi-modal mechanical approach to training monitoring in elite professional soccer. Science and Medicine in Football, 3938(July), 1–6.
- Rago, V., Rebelo, A., Krustrup, P., & Mohr, M. (2019). Contextual Variables and Training Load Throughout a Competitive Period in a Top-Level Male Soccer Team. Journal of Strength and Conditioning Research, (25), 1.

Berni Guerrero-Calderón
S&C Coach | Rehab Therapist | Sport Scientist
If you have any doubt, do not hesitate to leave your comment. If you liked the post, share it on social media!
All the information of this post has been retrieved from the paper published in Soccer & Society Journal.






Last comments